“Knee pain toh age ke saath hota hi hai.”
This is one of the most common—and most misleading—statements we hear in clinic.
While ageing increases the risk of joint problems, knee pain is never just about age.
It is about which structure is involved, how it is loaded, and what other clues the body is giving.
Why Knee Pain Needs Proper Evaluation
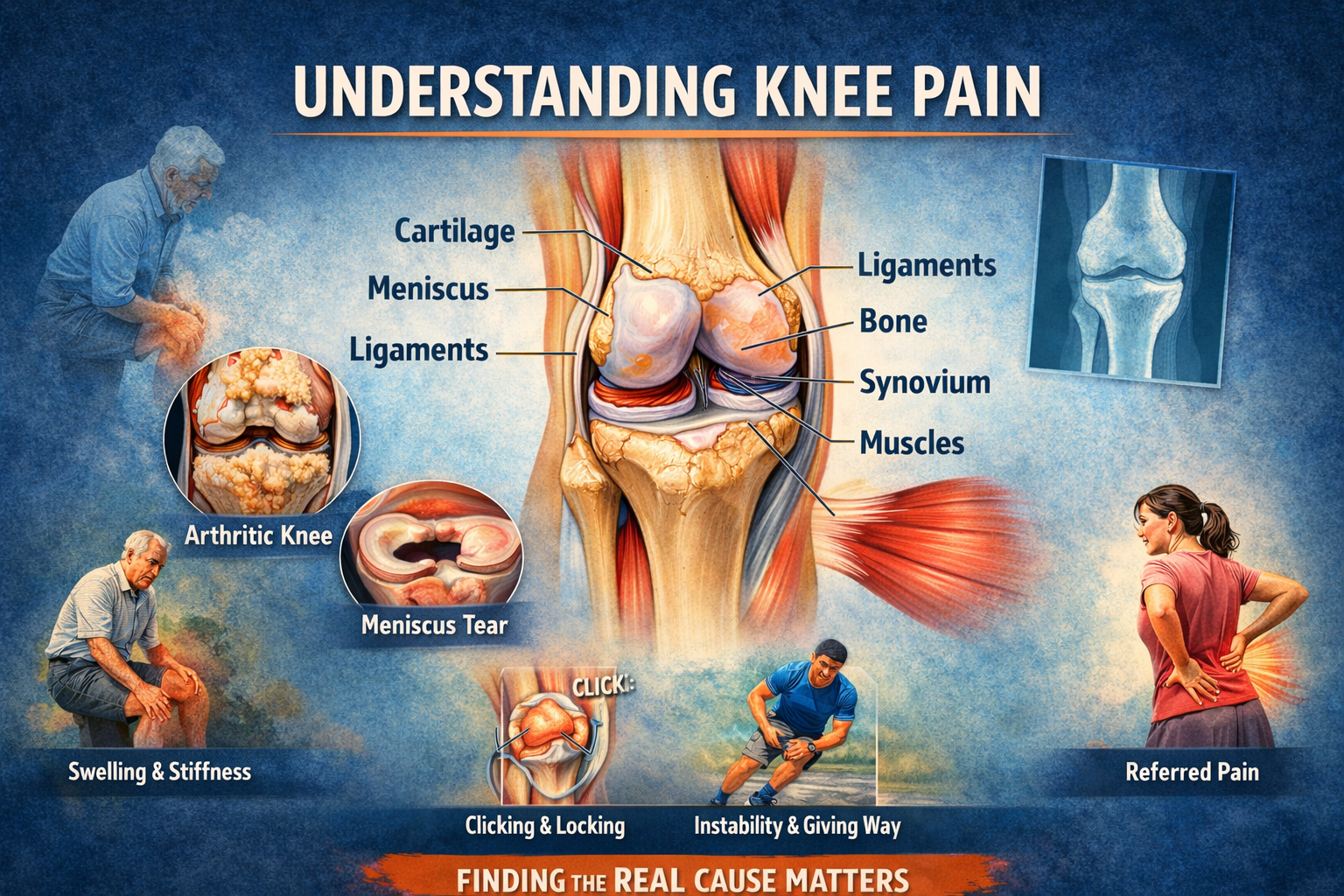
The knee is a complex joint involving:
- Cartilage
- Meniscus
- Ligaments
- Bone
- Synovium (joint lining)
- Surrounding muscles
Pain can originate from any one—or several—of these.
That is why the pattern of pain often matters more than the intensity.
Common Knee Pain Patterns Doctors Look For
| Symptom / Pattern | Likely Cause | Clinical Pointer (Why it Matters) |
|---|---|---|
| Pain while getting up from sitting, stairs, squatting | Chondromalacia / Patellofemoral pain | Cartilage under kneecap is load-sensitive |
| Clicking, locking, feeling something “stuck” | Meniscus tear | Mechanical symptoms suggest intra-joint pathology |
| Bowed legs with increasing pain over years | Osteoarthritis | Alignment + cartilage degeneration |
| Morning stiffness >30–60 minutes, multiple joints involved | Rheumatoid arthritis | Inflammatory, systemic disease |
| Sudden painful swelling with fever | Joint infection (Septic arthritis) | Medical emergency |
| Swelling after minor trigger or infection elsewhere | Reactive synovitis / Reactive arthritis | Often associated with gut/urinary infections |
| Knee pain with back pain or hip pain | Referred pain | Knee may not be the primary problem |
| Instability, giving way | Ligament injury (ACL/PCL) | Functional deficit, not just pain |
Important: No single symptom gives the full answer — doctors interpret patterns, not isolated complaints.
How Orthopaedic Doctors Actually Diagnose Knee Pain
- Listening Carefully to the Story
We look for:
- When pain started
- What activity worsens it
- Swelling pattern
- Night pain
- Other joint involvement
- Recent infections or fever
Often, the diagnosis begins before any scan.
- Clinical Examination
A hands-on exam helps assess:
- Swelling and warmth
- Range of motion
- Stability of ligaments
- Alignment of legs
- Muscle strength and balance
Many conditions can be suspected without imaging at this stage.
- Targeted Investigations
Tests are chosen to confirm a suspicion, not to “look for something”.
- X-rays → arthritis, alignment, bone changes
- MRI → meniscus, ligaments, cartilage, synovium
- Blood tests → inflammatory or infectious causes
Ordering unnecessary scans often creates confusion, not clarity.
Why Early Diagnosis Makes a Difference
Ignoring knee pain or self-treating for months can lead to:
- Progression of damage
- Muscle wasting
- Loss of confidence in movement
- Avoidable surgery later
Early diagnosis allows:
- Rehab-first strategies
- Medical management
- Lifestyle correction
- Surgery only when truly indicated
A Word of Caution About “Ageing”
Ageing explains risk, not cause.
Two people of the same age can have:
- Completely different knees
- Different pain thresholds
- Very different treatment needs
Good orthopaedic care is individualised, not age-based.
Take-Home Message
Knee pain is a signal, not a sentence.
Understanding why it hurts — early and correctly — often prevents bigger problems later and helps patients regain confidence, mobility, and quality of life.